Source: http://www.primehealthchannel.com/nasopharyngeal-carcinoma.html
Firstly, it is an honour to write in a premier issue of medical writing for the public. In this posting, I hope to share my experience dealing with nasopharyngeal carcinoma or cancer of nasopharynx, seen at my current setting in both Sabah & Sarawak. This is my simplified version merged with my personal experience. However, if you need straight facts- the web will cater better to your needs. Most people are not aware of such cancer. Most people do not know where the nasopharynx is.
Even most medical students don’t know where the boundaries of nasopharynx are. Most students will only have 2 weeks posting of ENT- most days will be spent on tonsillitis, discharging ear, hoarse voice, etc. Worse if they are trained overseas without ever seeing a single NPC patient, especially in non endemic areas. This further illustrates how little our medical professionals were emphasized on cancer of nasopharynx.
Nasopharynx, basically is the deepest area of the nose, just before the entrance into back part of the mouth. When we break bad news to our patients- we will tell them- ‘kanser belakang hidung’ (cancer at the back part of the nose). Due to the location, this cancer usually has late presentation, as not visible from external view. In 2007 National Cancer Registry, nasopharyngeal cancer is the fourth common cancer among population; after breast, colorectal & lung cancer. It is more common in male and patients of Chinese origin, comparatively to Malay, and very rarely in Indian population.
In the same registry, NPC was the most common cancer in Sarawak male and third most common cancer in Sabah male population. Previous study conducted in Sarawak, the incidence of NPC is comparatively as high as those from Southern Province of China, which happens to be the highest in the world. This is common among the Bidayuh, Iban, Kadazan, Dusun & other local pribumi in East Malaysia. In my current hospital in Kota Kinabalu, we see an average 3 new cases per week, which is comparatively high comparing to West Malaysian hospitals.
Source: http://www.macmillan.org.uk/Cancerinformation/Cancertypes/Headneck/Typesofheadneckcancers/Nasopharynx.aspx
The cancer has a strong genetic link, which makes it more common to occur within the same race. It also tends to run in families, among siblings. The Ebstein Barr Virus (EBV) has a common occurrence among NPC patients, but then again, it is also endemic amongst our population, and so far the vaccination for EBV is still at research level. Unfortunately, NPC is not as glamorous as breast or colorectal cancer where adequate amount of funds are poured into developing vaccines and oncological drugs. We are still lagging in prevention & treatment aspects. Hopefully our Oriental counterparts are coming close to clinical trials.
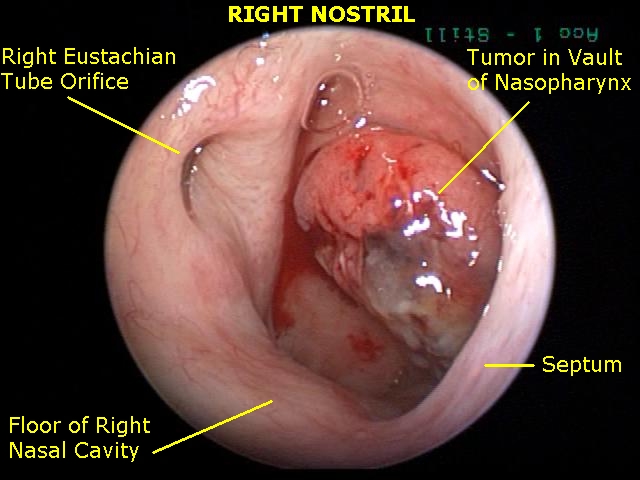
You may ask, how does this cancer manifest itself? The cancer starts at a crease in the nasopharynx called the Fossa of Rossenmuller. This area is next to the Eustachian tube opening, which connects the ear to the nose. Once the tumour enlarges, it will grow forward into the nostril, downwards into the sides of the mouth & throat. Also, it extends upwards through the crevices at the base of skull & ultimately into the floor of the brain. As with other carcinoma, this cancer will spread via lymphatic drainage into the cervical region. The cancer has the propensity to metastasize or spread to distant organs- typically lungs, liver and bone. The patient will initially complain of blocked ear, typically one sided, described as hearing loss similar when having a runny nose. The person will also experience bleeding from the nose and if tumour large, nasal blockage may occur. Once the tumour extends into skull base, the cranial nerves will be affected. An array of neurological symptoms may occur- reduced vision, squint, numbness of face, difficulty in swallowing, hoarseness of voice are among the common ones. Excruciating headache is a late symptom once the tumour has filled up the floor of the brain making it into a space occupying lesion.
The symptoms however, do not come in any particular order. Some may not have all the mentioned features. Some will only have neck swelling, usually on the sides, and painless. We have seen patients coming in with huge neck masses as large as a bowling ball before seeking any treatment. If there is an area of dead tumour cells- the skin will break and an area of discharging pus will occur and will leave the patient with a foul smelling fungating tumour at the neck. In late cases, the patient will have metastatic symptoms at distant organs. In rare cases, it may be the only presentation.
I recall during my early ENT medical officer days in Sarawak GH, where a young male chap was admitted to Orthopaedic Ward with paraplegia- unable to move both lower limbs. Diagnosis made was lumbar vertebrae pathological fracture most likely of distant metastasis. We were referred for possibility of NPC in view of trivial history of epistaxis months prior. Our nasal endoscopy revealed a very small mass in nasopharynx and our biopsy later did confirm it was NPC.
Last year, we also had a male patient presented to General Surgery for mild abdominal pain & later revealed a small liver mass. He was investigated with various scans and finally a liver biopsy revealed it was metastatic tumour. Also, he had very vague history of NPC. True enough, he had a nasopharyngeal mass which subsequently revealed to be NPC. Also we have seen few cases resembling lung cancer which turned out to be NPC in the end.
I hope to highlight to medical practitioners and public as well to be aware on the various presentations of NPC. It is also difficult to convince the public that the disease they have in their neck, ears or other body areas is actually coming from the back of the nose.
As this is too much to digest, I will look into investigations & other issues regarding NPC in my next write up.
[This article belongs to The Malaysian Medical Gazette. Any republication (online or offline) without written permission from The Malaysian Medical Gazette is prohibited.]